
‘Burning the Temple’ and Better Hospice Bereavement Care

In 2017, I went to Burning Man, a festival of the arts (not music) that takes place in the Nevada desert.
I had gone through a series of major changes in my life around that time, including my youngest daughter going away to college. Very little in my life at that time was the same as it was before. I did keep my beard though.
So I thought attending Burning Man, a ritual of “creative destruction” and reflection on the temporary nature of existence, would make for a good punctuation mark on my past and a springboard for the future.
It was not a mid-life crisis! Even from afar, the event had an influence on my life. Around 2008 I had gotten involved in the Chicago “burner” community, which fostered investment in the arts, community involvement and charitable work – as well as a good deal of fun. I built many lasting, close friendships through that community. It jumpstarted my creativity and exposed me to many new ideas. So I thought I should actually go there at least once, and this seemed like the right time.
The hallmark of the event is the burning of a massive wooden structure shaped like a man, which was kind of an awesome display as well as a boisterous celebration. However, Burning Man doesn’t end there. It culminates the following night with what is called the temple burn.

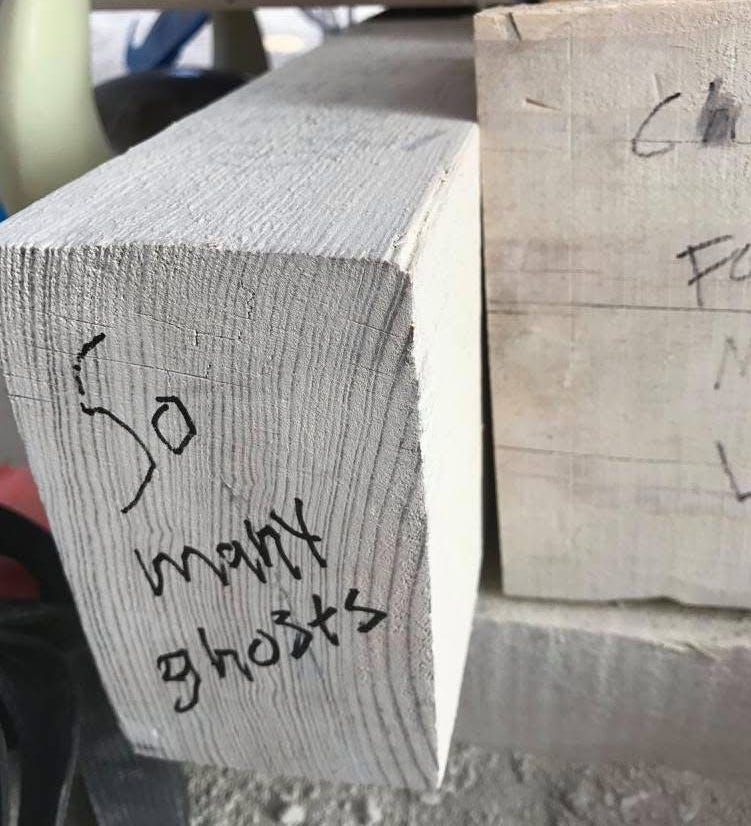
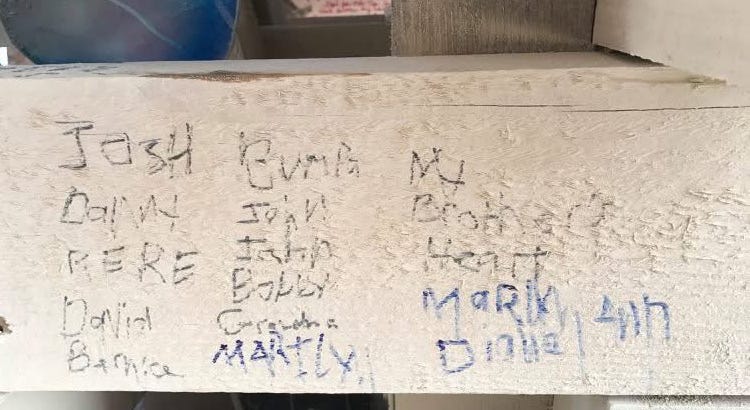
The temple, which has no religious affiliation whatsoever, is a place to grieve, reflect on loss and major life changes. Visitors are permitted to write messages on the walls and leave objects, often of great significance, to go up in flames as a ritual of letting go. In the temple I saw things like wedding dresses and military uniforms left to burn, as well as thousands of messages of both hope and renewal and expressions of deep pain.
As for me, I wrote the names of my lost loved ones on one corner of the wall and placed a wedding ring I no longer needed on the ground inside the temple.
The burning of the temple was a profoundly moving experience. While the burning of the man was a big, loud party, at the temple burn, literally tens of thousands of people gathered in silence. I heard no one speak, no cheers, no sound except the roaring of the flames. Around me people were holding hands and holding each other, and many were crying quiet tears.
I attended the burn alone, and I was struck by a deep catharsis. I wept, overcome with grief and anger, fell to my knees and I punched the sandy desert ground. Even though I was some distance away from the fire itself, I could feel the heat on my face. After all, this was a building-sized structure on fire.

The temple burn didn’t solve my problems or erase my grief, but it did acknowledge and honor it through a kind of ritual. Afterwards, I felt lighter, as though I had expunged something dark for at least a while.
I ended up walking over to one of the French camps and drinking a couple glasses of good red wine and had great conversations with a man from Ireland, a woman from Singapore, a couple from Denmark and two older adults I happened upon who lived 20 minutes away from me back home. Small world.
The temple got me thinking about the ways we process grief, which I really had never done. I held on to it like a cruel treasure. Would it dishonor my loved ones if I felt better, if I just accepted this? Shouldn’t someone feel bad – and in some cases angry – that they were gone? I had decided that person should be me. I had to carry this for their sake.
Perhaps I could have benefited from bereavement care from a hospice. Hospices hold families’ hands through their first year after a loss, as an extension of their mission and compliance with a regulatory requirement.
The problem that we have to acknowledge is that not all hospices do this well. While many offer direct, in-person or telehealth counseling, support groups, grief camps for children, workshops and other programs, others simply send out a monthly mailer or the occasional phone call. It can be pretty uneven from provider to provider.
Bereavement care, along with chaplain services, is among the least regulated and loosely defined aspects of hospice care. No guidelines or requirements specify what grief services should look like. Hospices have to define and design their programs on their own, and some do it better than others. Hospices really don’t get paid for it either, so they do this with no business incentive or support.
A 2013 study found that 78% of hospices provide bereavement care to patients’ families and 76% offer these services to the larger community regardless of whether the deceased had utilized their services. I can’t even guess at what’s going on with the 22% that apparently don’t provide this care.
However, only 23% of hospices provide “labor-intensive” grief services, and 27% offer “comprehensive care,” according to this research. Larger hospices appear more likely to offer labor-intensive or comprehensive care, the study found, and no significant differences were identified by ownership type. Although, nonprofits were more likely to offer care to the larger community rather than strictly to the families of their patients.
“Our results demonstrate substantial diversity in the scope and intensity of services provided to families of patients with terminal illnesses, suggesting a need for clearer guidance on what hospices should provide to exemplify best practices,” the study authors concluded. “Consensus within the field on more precise guidelines in this area is essential.”
More recent research from 2025 indicated that a family’s experience with grief greatly influences their perceptions of the end-of-life care their loved ones received. Also, high-quality care itself helped family members cope with their losses.
Also, thanks to reader Jerry Soucy who got me thinking about this with a comment on another post.
“Bereavement support is as wildly variable among hospices as everything else, there are too many crappy and mediocre hospices providing crappy and mediocre psychosocial support,” he said. Good point.
I urge hospices to take a sharp look at their bereavement programs to ensure they are robust and able to meet families needs. Could you be doing better? Could you be doing more? And what kind of determination and resources would you need in order to improve?
Also, as policymakers mull various payment reforms, such as altering the per diem structure or introducing payments for high-acuity palliative services, perhaps they should also consider some type of reimbursement and quality measures for bereavement care, beyond the Consumer Assessment of Health Care Providers and Services surveys.
Hospices of course can’t take away a person’s grief – even if they want to – but they can help, and families and loved ones need that help.
I’ve never heard of Burning Man before. Very interesting. Grief is so deeply personal as is bereavement. As for hospice is taking a sharp look at themselves (could you be doing better? Could you be doing more?) - this is a valuable exercise for all aspects of care delivery and for all hospice services, not just bereavement services.
"I urge hospices to take a sharp look at their bereavement programs to ensure they are robust and able to meet families needs. Could you be doing better? Could you be doing more? And what kind of determination and resources would you need in order to improve?"
.
You've got to get back to the basics - there are only 4 best practices for making money (making MONEY!) in hospice, and you've run right up against relentless cost-cutting
The vast majority of currently operating hospices are run to generate a financial return for investors, and they're not going to spend a penny that they don't explicitly and reluctantly have to
If there was anything crappy about your hospice experience, and it appears so at least in this regard (which is extremely critical, quite frankly - the deceased's problems are mercifully over but not for those of us left behind), then sadly your experience was typical for the vast majority of patients and families - the real world consequence of "mediocre hospice care"